CC: Mr. C is a 57-year-old man who complains of dysuria that started suddenly 5 days ago.
He reports the pain seems to radiate to his low back and perineum. He has felt “achy” and had chills but has not measured his temperature. He denies any penile discharge, rash, nausea, vomiting, or flank pain. He has had more difficulty urinating with a weaker urinary stream for the past few days. He also feels some dizziness upon standing.
Mr. C is sexually active with several female partners and does not use condoms or other barrier protection. He has no active medical problems but has noted nocturia over the past few months.
Temperature is 38.2°C, pulse 80 bpm, RR 12 breaths per minute, BP 142/78 mm Hg, and orthostatic vital signs are negative. Abdominal exam demonstrates suprapubic tenderness without rebound or guarding and the absence of CVA tenderness. Genital exam is normal, but there is tenderness on gentle prostate exam without any palpable masses.
Mr. C’s urinalysis is positive for leukocyte esterase, 10 WBCs per high power field, and occasional blood with 5 RBCs per high power field. His CBC shows a WBC count of 8.0 K/mcL and basic metabolic panel shows a creatinine of 1.0, similar to his previous baseline.
Mr. C was treated empirically with ciprofloxacin, 500 mg twice daily, and azithromycin, 1 g for 1 dose, for acute bacterial prostatitis. Results of the urine culture showed 150,000 colony forming units of E coli susceptible to fluoroquinolones. The urine PCR for gonorrhea and chlamydia was negative. Treatment with ciprofloxacin was continued for 21 days, and his symptoms resolved. He continued to have nocturia and treatment for benign prostatic hypertrophy was started.
SOAP note
S: 57 year old male presents with dysuria for the past 5 days, with pain radiating to his lower back and perineum. Admits to nocturia over the past few months, feeling “achy”, having difficulty urinating with a weaker urinary stream, and dizziness while standing. Denies penile discharge, rash, nausea, vomiting or flank pain.
O: BP – 142/78 mm Hg
P – 80 bpm
RR – 12
Temperature – 38.2 °C
Orthostatic vital signs negative
Abdominal exam shows suprapubic tenderness without rebound or guarding. No sign of CVA tenderness. Normal genital exam. Tenderness on prostate exam with no palpable masses. Urinalysis is positive for leukocyte esterase, 10 WBCs per high power field, and blood with 5 RBCs per high power field. CBC shows WBC count of 8.0 K/mcL and BMP shows creatinine of 1.0.
Urine culture 150,000 colony forming units of E.coli
Urine PCR negative for chlamydia and gonorrhea
A: Acute Prostatitis
Ddx – urosepsis, complicated cystitis, urethritis from STI
P: Ciprofloxacin 500 mg twice daily for 21 days, azithromycin 1 g for 1 dose. Symptoms resolved after the 21 days. Patient continued to have nocturia and treatment for benign prostatic hypertrophy started.
Summary
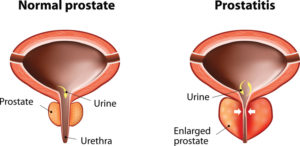
Mr. C is having symptoms of dysuria with radiation to the perineum and urinary hesitancy, all of which point to acute prostatitis. Acute prostatitis presents with dysuria, lower back pain, perineal pain, fever, chills and myalgias. Patients may also have symptoms and urinary frequency, urgency or obstruction. Acute bacterial prostatitis is an infection of the prostate gland that occurs though reflux of urine into the prostate or from an ascending urethral infection. Possible causes include gram-negative coliform bacteria, Klebsiella, Proteus, enterococci, Pseudomonas, or Chlamydia. Diagnosis for acute prostatitis is made based on a combination of history, physical exam and urine studies. Findings on urinalysis with the tender prostate physical exam support the diagnosis of acute prostatitis as opposed to cystitis or urethritis. Urethritis from STI was likely, given the patient is sexually active with several female partners without the use of condoms or other protective barriers. Urethritis presents with dysuria, urethral pruritis, penile discharge, testicular and abdominal pain, and dyspareunia. The negative PCR result of chlamydia and gonorrhea and absence of penile discharge made the differential diagnosis of urethritis unlikely. A differential diagnosis of urosepsis is unlikely given the vital signs and absence of SIRS criteria (WBC >12,000 K/mcL or WBC <4,000 K/mcL, temperature of >38.0°C or <36.0°C, tachycardia >90 bpm or tachypnea >20 breaths per minute).

This entry is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International license.